58 years old farmer with pedal edema
This is an E log book to discuss our patient's de-identified health data shared after taking his guardian's signed informed consent. Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable comments in comment box are most welcomed
I have been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency I reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Stimita Maity
Short case
H tckt no 1701006178
Chief complaints
58 year old male resident of suryapet farmer by occupation came with chief complaints of
Edema in both the legs and pain in the loin region since 5 days
History of present illness
Patient was apparently asymptomatic 5 days ago then he developed pedal edema in both the limbs till ankle which is of pitting type, Insidious in onstet gradually progressive,no aggravating and relieving factors.
Pain in loin region - dull aching type,continuous pain,not associated with any aggravating and relieving factors, no radiation of pain.
History of joint pain, back pain.
H/o easy fatiguability, stiffness of proximal muscle.
H/o burning micturition, nocturia.
No h/o orthopnea,PND
He was diagnosed with chronic kidney disease 1 year ago and has undergone 4 sessions of dialysis.
Last 6 month he had not undergone any session of dialysis.
No history of fever chills or rigors.
No history of NSAIDS abuse.
No h/o anorexia, nausea,metallic taste in mouth.
No h/o anuria


Past history
No history of Hypertension Diabetes Bronchial Asthma Epilepsy thyroid tuberculosis
Family history
Not relevant
Personal history
He takes mixed diet
Appetite normal
Bowel and bladder movements are regular
Non smoker
Occasional alcoholic
No known allergies
General examination
Well informed consent is taken. Examined in a well lit room.
Patient is conscious coherent and coperative well oriented to time place and person.
Moderately built and moderately Nourished.
Vitals
Afebrile
BP 110/70mmhg
PR 90bpm
Respiratory rate 18 cpm
There is mild pallor, but no icterus, clubbing, cyanosis or lympathadenopathy.
Bilateral pedal Edema pitting type upto ankle.


Systemic examination
Abdominal examination
INSPECTION:
•Shape – scaphoid
Flanks – free
Umbilicus –central in position , inverted.
All quadrants of abdomen are moving equally with respiration.
No dilated veins, hernial orifices, sinuses
No visible pulsations.
PALPATION:
•No local rise of temperature and tenderness
All inspectory findings are confirmed.
No guarding, rigidity
Deep palpation- no organomegaly.
PERCUSSION:
•There is no fluid thrill , shifting dullness.
Percussion over abdomen-
tympanic note heard.
AUSCULTATION:
Bowel sounds are heard.
Cardiovascular system examination
INSPECTION:
•Chest wall - bilaterally symmetrical
No dilated veins, scars, sinuses
PALPATION:
•Apical impulse is felt on the left 5th intercostal space 1cm medial to mid clavicular line.
No parasternal heave, thrills felt
AUSCULTATION:
•S1 and S2 heard , no added thrills and murmurs heard.
Respiratory system examination
INSPECTION:
•Chest is bilaterally symmetrical
Trachea – midline in position.0
Apical Impulse is not appreciated
Chest is moving normally with respiration.
No dilated veins, scars, sinuses.
PALPATION:
•Trachea – midline in position.
Apical impulse is felt on the left 5th intercoastal space.
Chest is moving equally on respiration on both sides
Tactile Vocal fremitus - appreciated
PERCUSSION:
The following areas were percussed on either sides-
Supraclavicular-resonant
Infraclavicular- resonant
Mammary- resonant
Axillary- resonant
Infraaxillary- resonant
Suprascapular- resonant
Infrascapular- resonant
interscapular - resonant.
AUSCULTATION:
•Normal vesicular breath sounds heard
No adventitious sounds
Central nervous system examination
HIGHER MENTAL FUNCTIONS:
•Patient is Conscious, well oriented to time, place and person.
All cranial nerves - intact
•Motor system: Intact
Superficial reflexes and deep reflexes are present , normal
Gait is normal
No involuntary movements
•Sensory system -
-All sensations pain, touch,temperature, position, vibration, are well appreciated.
Investigations
Serum iron 63 ug/dl



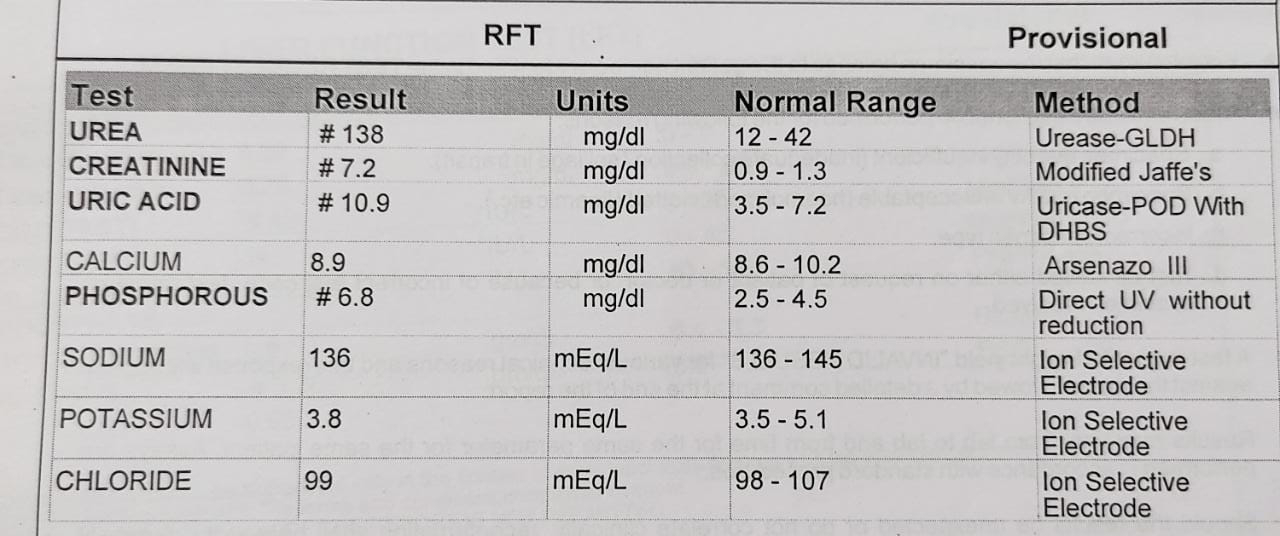

SGOT 43 IU/L(raised)
Alp raised 325 IU/do,Albumin deceased 3.36 gm/dl

HUV non reactive

HbsAg negative

Anti HCV antibody non reactive


Bilateral trade 2-3 RPD with simple renal cyst




{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment